- Language

Kimmatkar1, V. Thawani2, L. Hingorani3, and R. Khiyani4
1 MS Orthopedics, Indira Gandhi Medical College, Nagpur, India
2 MD Pharmacology, Government Medical College, Nagpur, India
3 PhD Pharmaceutical Sciences, Pharmanza (India), GIDC, Kansari, India
4 MD PhD, Ayurveda, Government Ayurvedic College, Nagpur, India
Summary
Osteoarthritis is a common, chronic, progressive, skeletal, degenerative disorder, which commonly affects the knee joint. Boswellia serrata tree is commonly found in India. The therapeutic value of its gum (guggulu) has been known. It posses good anti-inflammatory, anti-arthritic and analgesic activity.
A randomized double blind placebo controlled crossover study was conducted to assess the effi-cacy, safety and tolerability of Boswellia serrata Extract (BSE) in 30 patients of osteoarthritis of knee, 15 each receiving active drug or placebo for eight weeks. After the first intervention, washout was given and then the groups were crossed over to receive the opposite intervention for eight weeks. All patients receiving drug treatment reported decrease in knee pain, increased knee flexion and increased walking distance. The frequency of swelling in the knee joint was de-creased. Radiologically there was no change. The observed differences between drug treated and placebo being statistically significant, are clinically relevant. BSE was well tolerated by the subjects except for minor gastrointestinal ADRs. BSE is recommended in the patients of os-
teoarthritisosteoarthritis of the knee with possible therapeutic use in other arthritis.
Key words: Boswellic Acid (BA), Boswellia serrata Extract (BSE), Osteoarthritis of knee (OA knee), Non Steroidal anti-inflammatory Drugs (NSAIDs), Adverse Drug Reactions (ADRs)
Introduction
Osteoarthritis of the knee (OA knee) is a common, chronic, progressive, skeletal, degenerative disorder. Despite continued physiotherapy and wide use of non-steroidal anti-inflammatory drugs (NSAIDs), this dis-ease is of concern since it affects the mobility of indi-viduals and their quality of life. The NSAIDs mainly act by blocking prostaglandin synthesis. The other me-diators of inflammation like leukotrines and comple-ment pathways are not influenced by the NSAIDs. Therefore the search has been on to find a better alter-native. Globally, currently there is greater interest in non-synthetic, natural drugs derived from plant/herbal sources due to better tolerance and decreased adverse drug reactions (ADRs).
Boswellia serrata, in Sanskrit is known as Gajabhak-shya, implying its ingestion by elephants. Charaka, Bhavamisra and others have described it as useful. It grows widely on dry hills of northwest India. It posses anti-inflammatory, anti-arthritic and analgesic activity (Selected Medicinal Plants of India, 1992).
Boswellia serrata is a tree of moderate height, which grows in hilly areas of India. The therapeutic value of dried resinous gum (guggulu), derived from tapping the Boswellia tree has been known since antiquity.
Boswellia gum has been mentioned in the ancient Ayurvedic texts Sushrita Samhita and Charaka Samhita (Kulkarni et al., 1991). The gum resin of the Boswellia serrata has been used for the treatment of the inflammatory disease in the traditional Ayurvedic medicine in India (Kirtikar and Basu, 1935; Chatterjee and Pal, 1984). Gum resin extracted from Boswellia serrata posses good anti-inflammatory, anti-arthritic and analgesic ac-tivity, significantly reducing the total WBC count in the joint fluid, restoring the integrity of blood vessels oblit-erated by spasm or internal damage (Altern. Med. Rev. 1998; Kulkarni et al. 1991). However there is lack of supporting studies regarding the effect of BSE in the treatment of OA knee. Therefore the present study was planned to assess the efficacy, safety and tolerability of BSE in OA knee.
Materials and Methods
Study design
This was a randomized double blind placebo controlled crossover study of 30 patients attending the out patient department of Orthopaedics in Indira Gandhi Medical College, Nagpur, India.
Patients
Patients above the age of 40 years of either gender, with clinicoradiological osteoarthritis of knee, taking physiotherapy and any NSAIDs, were identified and approached to participate in the study. Patients with history of peptic ulcer or acid peptic disease, hypersen-sitivity to NSAIDs, pregnant or breast feeding women, having concomitant disease, taking concurrent medica-tion, having end stage organ damage or those who had
received corticosteroids within 4 weeks/other anti-in-flammatory analgesics within 3 days prior to enroll-ment and having other concurrent diseases were ex-cluded from the study.
Informed consent was obtained from those who vol-unteered. They were subjected to a pre-tested, validated questionnaire to get relevant information about the walking distance, difficulty in kneeling down, sitting crossed legged and squatting. Patients with joint swelling were asked about the frequency of the joint pains. They were asked to grade the pain intensity on a 0 to 3 point visual analogue scale (0 = absent, 1 = mild, 2 = moderate, 3 = severe); loss of function on a 0 to 3 point visual analogue scale (0 = no loss of function, 1 = slight loss of function, 2 = moderate loss of func-tion, 3 = severe loss of function) and swelling on a 0 to 3-point visual analogue scale (0 = absent, 1 = mild, 2 = moderate, 3 = severe). Willingness for the change of the drug therapy was taken. They were discontinued from NSAIDs and given a wash out period of seven days. However they were allowed to continue with the physiotherapy, subject to no modification in routines. Radiographs of the affected knee joint were taken 1) initially, 2) at the end of the first intervention, 3) at the time of cross over and 4) at the end of the study.
Methods
Thirty patients were randomly allocated (randomiza-tion done by SAS system for Windows) in two groups of 15 each, to receive either active drug BSE of Salki Guggulu (Cap Wokvelä, manufactured by Pharmanza India) containing 333 mg of BSE per capsule, or place-bo containing starch powder (supplied by Pharmanza India) in matching blister packing, colour, shape and size of the capsules in the dose of one capsule three
times a day for eight weeks. Those who received BSE in first intervention were later crossed over to receive placebo in the second intervention and vice-versa. Each capsule of Wokvelä contained the standardized extract of Boswellia serrata gum having minimum 65% organic acids or minimum 40% total Boswellic Acids (BA). Main components of BA in BSE used were 11-keto-beta BA – 6.44%, 3-O-Acetyl-11-keto-beta BA – 2%, beta-BA – 18.51%, 3-O-Acetyl-beta BA – 8.58%, alpha BA- 6.93% and 3-O-Acetyl-alpha BA – 1.853%. Content analysis was done by HPLC-UV detector. Primary standards were used from Chro-maDex. All other chemicals were purchased from Merck in the highest available analytical grade. Since the active drug and placebo were dispensed in capsule formulation, masking the smell of active drug BSE, was not done. The clinical orthopedic investigator and the patients were blind for the interventions. Before starting and at the end, of first intervention as well as second intervention, the patients were asked to grade the pain intensity, loss of function and swelling. Radiographs were also taken at these points. Washout period of 21 days was given at the end of first interven-tion to ensure that the residual effect of the first inter-vention did not linger and affect the second one. After washout, the crossover was done, with each patient get-ting opposite of the previous intervention. The obser-vations were decoded, tabulated and then analyzed. The patients were stressed the importance of not miss-ing any dose and to record any such miss in the feedback form provided to them. They were asked to continue with the physiotherapy and inform intercurrent illness and ADRs, if any. They were given the assigned inter-vention for the duration of four weeks at a time and re-viewed after four weeks and asked to return the empty blister packs for getting refill at that time. Consumed capsule count was recorded to know the compliance. Compliance upto 80% of adherence to recommenda-tions was accepted as subject being compliant. These patients had unrestricted access to the investigators over mobile phone, referred status in meeting without prior appointment, free investigations and transport for self and companion during the study period.
Clinical evaluation
The evaluation of efficacy was in terms of decrease in the pain and swelling and improvement in the function at the end of the intervention. Pre and post intervention radiographs were also compared.
Statistical analysis
The demographic and other baseline characteristics of the patient enrolled in this study have been summerized in tables. The changes in pain intensity, swelling and loss of function scores from baseline to end points of in-terventions have been analysed doing Wilcoxon signed rank test with level of alpha set at 0.05.
Results
Patient Characteristics
The study population consisted of 12 men and 18 wo-men, aged between 45 and 72 years (mean age 59.03). Their body weight ranged from 49 kg to 79 kg (mean 69.41 Kg) and their height from 150 cm to 176 cm (mean 161.86 cm). There was no concurrent medical disease in any patient included in this study. No patient was on any concomitant medication during the study period. All the patients showed the compliance to the study.
Clinical efficacy
All patients were assessed for the severity of pain, swelling and improvement of function initially, at the end of the first intervention, at the beginning and end of the second intervention.
The mean scores for the efficacy variables obtained at the base line and after eight weeks of the first inter-vention are presented (Table 1). The decrease in severi-ty of pain and swelling and improvement in the loss of function were clinically and statistically significant (p < 0.001) in the group receiving the active drug as compared to the group receiving the placebo. At the second intervention after cross over, the patients showed the worsening of the above parameters in the group receiving the placebo and vice versa in the pa-tient receiving the drug (Table 2). There was no re-markable variation between the efficacy variable val-ues at the beginning of the first intervention and after crossover at the beginning of the second intervention.
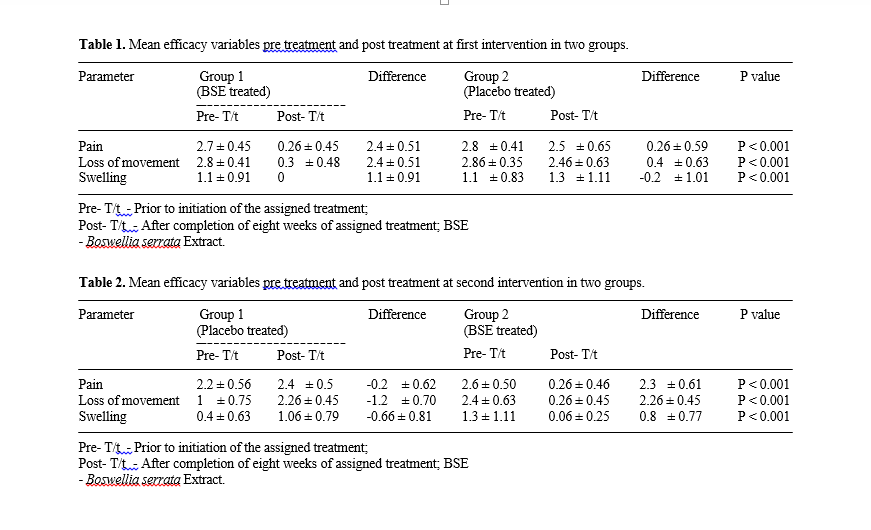
After the interventions in the group receiving the ac-tive drug, all patients reported decrease in knee pain, increased knee flexion, increased walking distance, im-provement in capacity of climbing stairs, better ability in kneeling, crossed legged sitting and squatting. The knee range of movement was improved. The frequency of swelling in the knee joint was decreased. Radiologi-cally there was no change.
Adverse effects
The ADRs of the BSE therapy included loose motions in one, epigastric pain and nausea in one, which re-sponded to usual symptomatic treatment. None of these two patients discontinued the drug because of the ADRs. General patient compliance to BSE was satis-factory. All patients chose to continue with the BSE treatment even after the completion of the study.
Discussion
Boswellia serrata trees grow in India. On stripping the bark, it yields a gummy oleoresin, which contains oils, terpenoids and gum. Up to 16 percent of the resin is es-sential oil, the majority being alphathugene and p-cymene. Four pentacyclic triterpene acids are also present, with beta-boswellic acid being major con-stituent. The therapeutic value of dried resinous gum also known as guggulu, has been known since antiqui-ty. Boswellia gum has been mentioned in ancient Indi-an Ayurvedic texts – the Sushrita Samhita and the Charak Samhita (Alt. Med. Review, 1998).
Animal studies performed in India show that inges-tion of a defatted alcoholic extract of Boswellia de-creased polymorphonuclear leukocyte infiltration and migration, decreased primary antibody synthesis (Sharma et al., 1988; Sharma et al., 1989) and caused almost total inhibition of classical complement path-way. In an in vitro study of effects of beta Boswellic acid on complement system, the extract demonstrated a marked inhibitory effect on both classical and alternate pathway of complement system (Knaus and Wagner, 1996). An investigation of Boswellia’s analgesic and psychopharmacological effects in animals found that it exhibited marked sedative and analgesic effect (Menon and Kar, 1971). Boswellic acid, a pentacyclic triter-penoid and its acetylated derivatives have effects on both the production of antibodies and cell mediated im-munity (Safayhi et al., 1992).
It has been suggested that the BSE is rich in BA iso-mers alpha and beta BA, 11-keto-beta BA and their acetyl derivatives (Krohn et al., 2001). These BAs are specific, non redox inhibitors of 5 -lipoxygenase and hence inhibit leukotrine biosynthesis in dose dependent manner (Safayhi et al., 1992). These acids decrease specifically the pro-inflammatory 5-lipoxygenase products including 5-hydroxyeicosatetraenoic acid (5-HETE) and leukotrine B4 (LTB-4) levels (Ammon et al., 1991), which being the active chemotactic fac-tors cause increased permeability (Robertson RP,1987). Hence, lesser number of the white blood cell army is recruited to the site of inflammation or trauma, thus dampening the inflammatory response, which leads to faster healing. NSAIDs can cause disruption of glycosaminoglycan synthesis, which can accelerate the articular damage in arthritic conditions. The BSE has been claimed to de-crease the glycosaminoglycan degradation (Reddyet al., 1989) which helps to keep the cartilage in good condition. This might be responsible for the recovery of the patients in OAand might stop progression of this condition.
The BSE has an effect on production of antibodies and cell-mediated immunity. It also inhibits human leukocyte elastase (HLE) (Safayhi et al., 1997). This could be of help in autoimmune disorders like rheuma-toid arthritis.
Our findings show that there is statistically signifi-cant improvement in the efficacy variables in the pa-tients of OA knee treated with BSE. After eight weeks of thrice daily administration in the dose of 333 mg per capsule, BSE decreased the pain in the affected knee joints, decreased the swelling and improved the loss of function in terms of increased knee flexion, stairs climbing and walking distance. Radiologically there was no change in the affected joints. BSE is recom-mended in the patients with OA knee and may also have therapeutic utility in the treatment of other arthri-tis like osteoarthritis of other joints, JRA, rheumatoid arthritis, ankylosing spondylosis and degenerative dis-eases of spine.
Acknowledgments
This paper forms the part of the required course work for “STA 101” Course in Fundamentals in Medical Statistics conducted by Lata Medical Research Foundation, Nagpur, India.
References
Address
Thawani, 14-A, Jeevan Jyoti, Clarke Town, Nagpur – 440 004, India
Tel.: ++91-712-522 977; Fax: ++91-712-559 060
Email: thawani@nagpur.dot.net.in
(Source: http://www.mchemist.com/proflexplus/pdf/boswellia%20serrata%207.pdf)